
In our ‘food obsessed society’ we are constantly bombarded by different trendy diets which often come with outlandish claims of great benefits. The one principle that professionals in the industry do seem to agree on these days is that there is no one diet that fits all. Thinking along the same lines, I have a strong interest in researching different diets and their applications, linking with nutrigenomics and functional testing, to ascertain which diets best fit a specific individual or athlete.
With genetic testing now easily accessible and affordable, I was keen to test my own profile in order to help determine my optimal dietary choice. I now know that I have genetic mutations that can predispose me to cardiovascular disease, late onset dementia and metabolic syndrome.
The ketogenic diet (KD) has been in clinical use for over 80 years primarily for the treatment of epilepsy1 symptoms, but recent scientific focus has been on its potential application in the field of neurodegenerative diseases and stroke recovery. It seemed a good fit for my genetic profile and hence my curiosity was sparked as to how the KD could be applied for health and in sport performance. That was my challenge – to see if I could make it work.
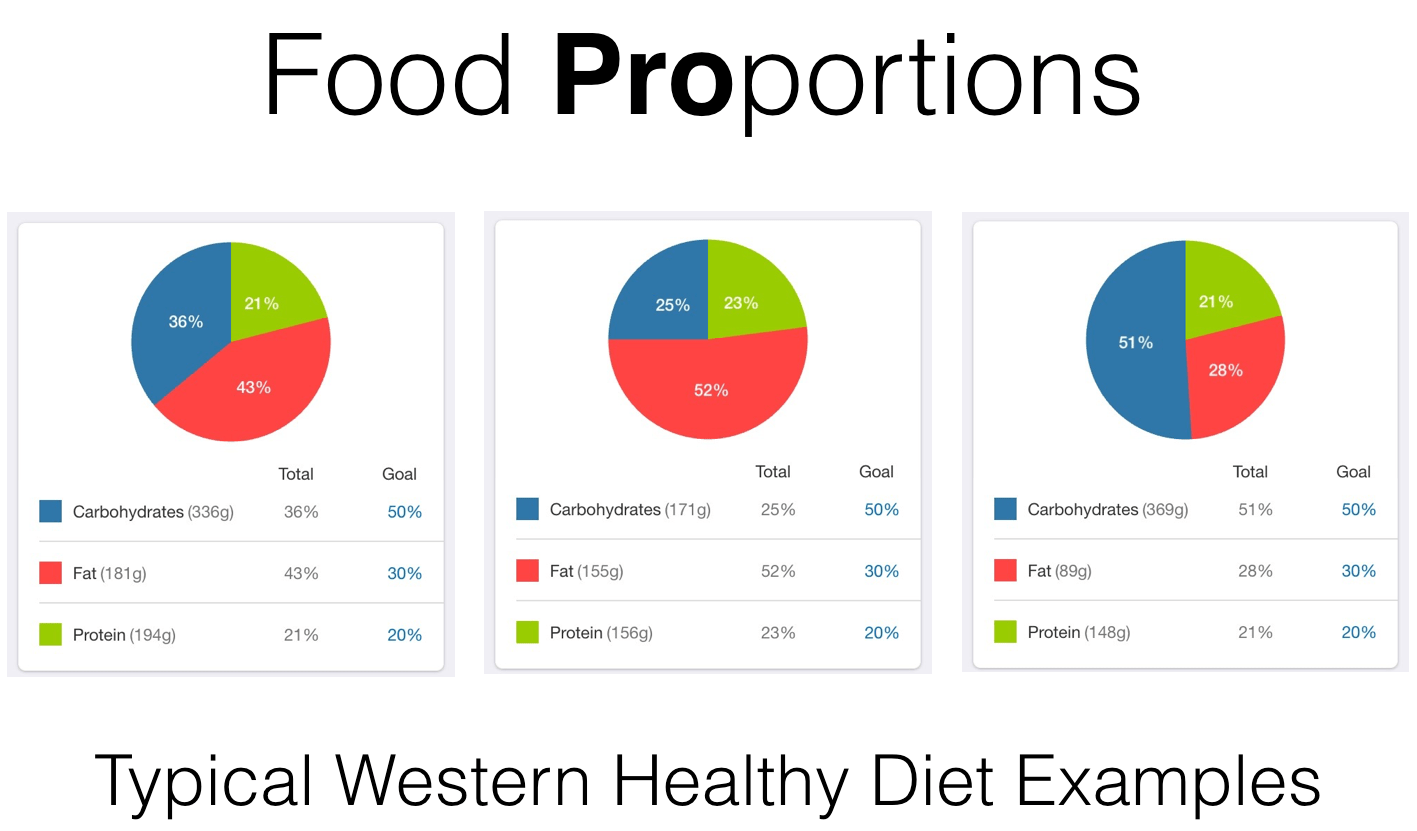
It’s important to understand the difference between a Low Carb High Fat diet (LCHF) and the Ketogenic Diet. The former could be ketogenic but does not have to be, whereas the latter is in all cases LCHF and normally medium protein (LCMPHF). I am slightly baffled why most articles, papers and blogs fail to mention protein in the KD – if protein levels are not taken into consideration this could end ketosis pretty quickly as around ⅓ of protein can enter gluconeogenesis and protein also could have a pretty strong insulinogenic effect. Although not as extreme, the LCHF diet could still lead to a benefit in performance as the individual is likely to cut out many foods that are generally negatively associated to health (sugars, refined and processed foods etc.). In addition, an increase in healthy fats can provide other metabolic benefits. My focus from this point is an investigation of ketosis, which will include these benefits and potentially many others. I will refer to that state as fat adapted (FA).
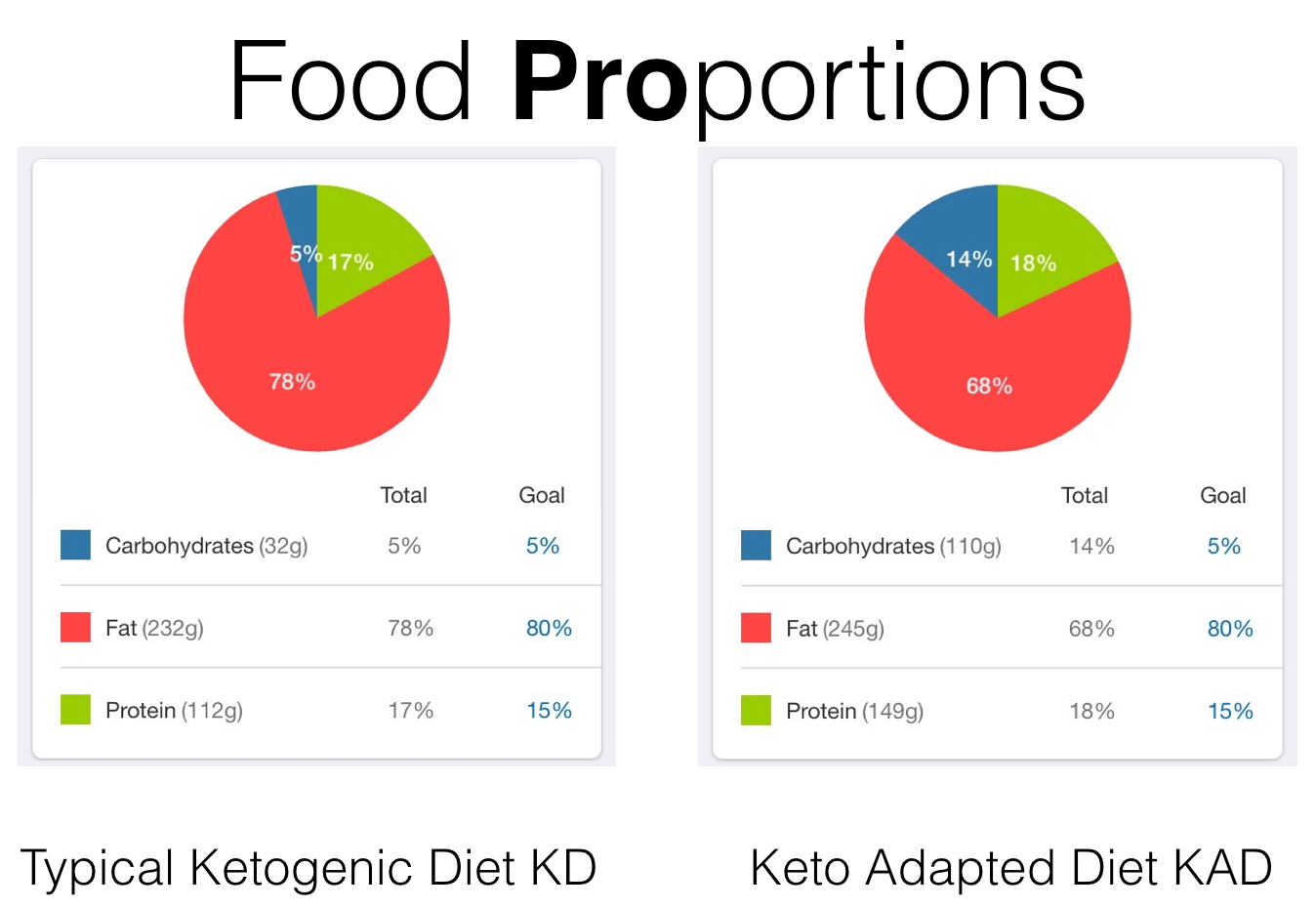
In general, the substrate proportions for Carbohydrates, Protein and Fats are:
I love data, I am one of those people that you do not want to ask what I do for living unless you too like data or you don’t mind having a very boring conversation! As it turns out, this love for data has proven to be really helpful in finding out different trends that have helped me to analyse specific applications in physiology.
When I started researching the Ketogenic Diet for general well-being and sports performance I noticed some very interesting trends. I had no preconceived ideas about whether the diet would or wouldn’t work for me and I decided to monitor as many variables as I could on a regular basis. The most important variables I measured were:
- heart rate variability (HRV),
- glycaemia,
- ketones,
- training intensity and duration for both aerobic and anaerobic sports,
- life load,
- sleep quantity and quality,
- morphometrics (like weight, body fat percentage)
- as well as blood tests including cholesterol (levels, particle size and number, insulin resistance, HCY, CPR Lp-PLA2).
Most of these parameters are pretty straightforward to measure and normally well known to most practitioners. HRV reflects the level of inflammation and sympathetic activation (stress load) on an individual and in a way is meaningless unless it is put into context. I see many people trying to get a higher HRV reading by changing breathing rate, posture or other ‘immediate’ environmental variables. I think this is pointless. HRV is a reflection of a body state, a mean number that quantifies what inflammation and sympathetic activation in the body at that moment in time. We need to act on the cause that is leading to the difference in the HRV reading.
We know that inflammation can be helpful in regenerating tissues to be stronger, faster and more resilient, but there is a point when it can become counterproductive. It’s the same with the stress response – sympathetic activation. Ideally we want to push as far as we can go with healthy inflammation and stimulus yet not to a point where it is damaging our performance and health. This is where HRV comes pretty handy in order to understand where the body is at.
I have been using HRV for many years and have found it very useful in understanding what degree of inflammatory response and sympathetic tone there is within the body compared to a relative baseline. After carrying out comprehensive testing on myself, I then decided to grab a bunch of guinea pigs to see whether their experiences would be similar. I also followed the work of scientists and researchers scattered around the world where who have been experimenting with ketogenic application and coming to have very similar results: Dr Peter Attia, Jacob Wilson PhD, Ben Greenfield and of course Prof Tim Noakes, Olympic coach.
As we know in ‘normal’ condition the body relies on glucose for most cell functions including energy production.
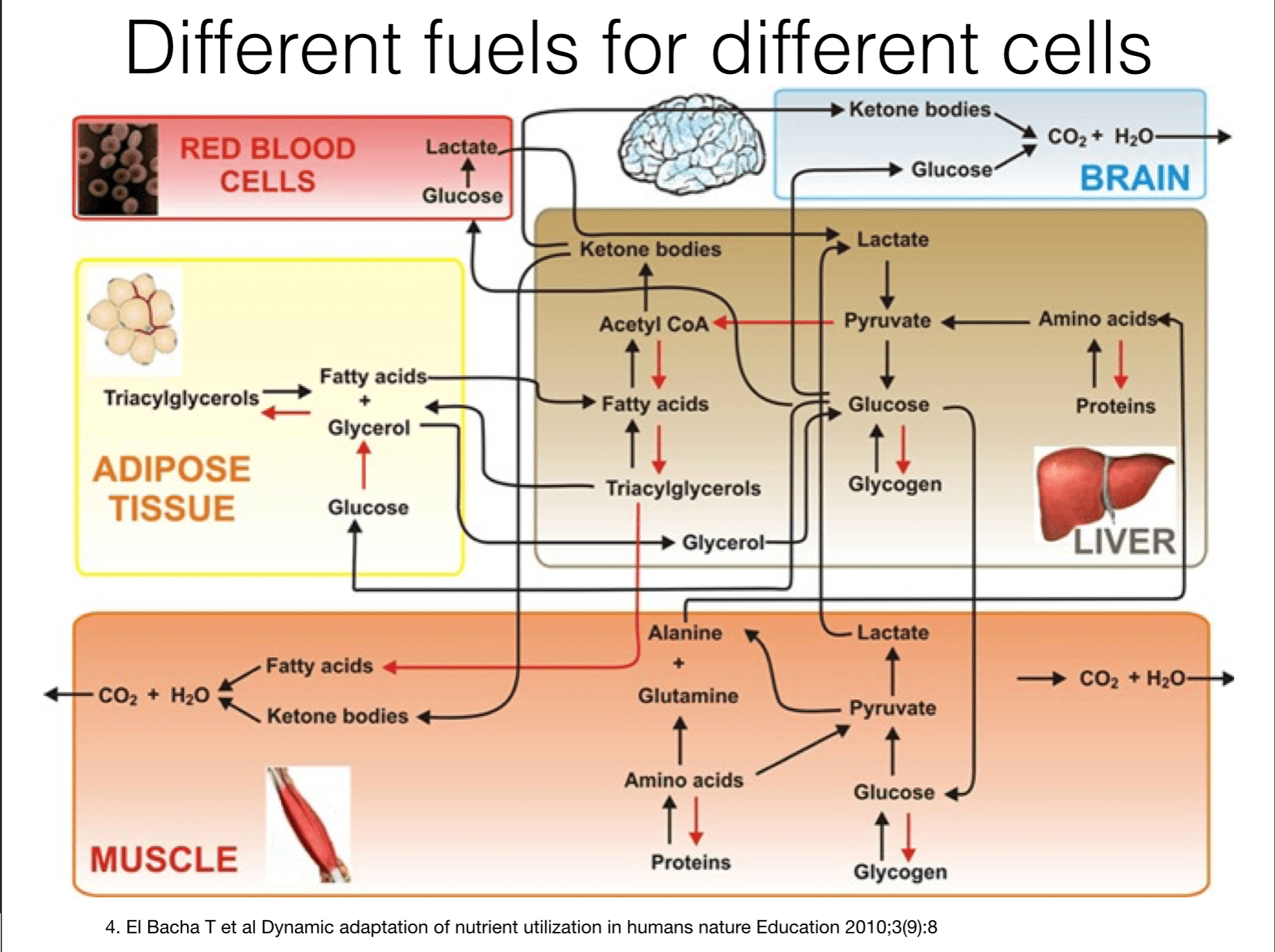
Especially in sport this is the main substrate that has been at the core of fuelling the body. We also know that in highly anaerobic conditions the body is forced to use glucose as burning fatty acids for energy takes too long and requires oxygen. See picture below.
The general consensus is that adaptation to a KD is quite tricky in the early stages and may include symptoms such as blood sugar dips, reduction in appetite and sporadic loose bowel movements. In addition, having large quantities of fats, including high levels of healthy saturated fats can present a psychological challenge. Will I get a heart attack? Have I increased my chances of a stroke? Will I have enough glucose to provide me with any energy? These recurrent questions kept myself and my group from getting bored! Needless to say we used a healthy dietary approach to a KD – with large portions of vegetables, fish, some very high quality grass fed meat, specific cooking methods and healthy post training smoothies. Everyone within my group, at least as far as I know, stayed away from highly refined junk food. It is paramount that this dietary approach is taken seriously as if it carried out without the due diligence it could be very dangerous not only from a sport performance perspective but also as a health in general. Interestingly there was a general consensus about how mental clarity improved past the adaptation period.
I allowed two months for the transition from a ‘healthy’ diet to a KD before I started to measure the variables described above. I knew from the research in recent years that a KD has been found to be very successful for specific diseases 2,3,4. Markers such as fasting glycaemia and blood/breath ketones improve, yet there is currently little evidence about other variables including HRV, life load and importantly, sports performance.
Three months into the testing we saw some noticeable improvements in the predominantly aerobic athletes. Amateurs reported benefits exceeding double-digit percentage figures in half marathons and cycling events, and semi-professional athletes also noted improvements. The KD took their performance time back to what it was years earlier, and in some cases to the best that they ever performed. There was a reduction in that ‘bonking out’ feeling across both groups. This makes perfect sense as ketones can be burnt efficiently in an oxygen rich environment.
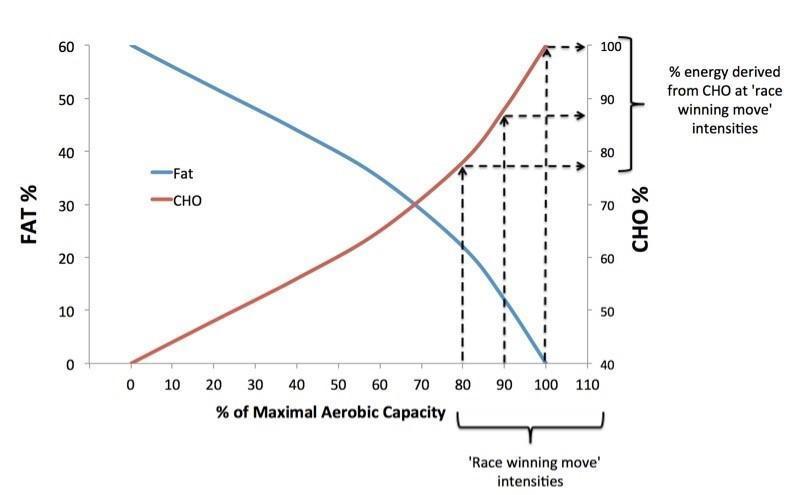
These findings are totally in line with the FASTER study which showed that people that are fat adapted when challenged at 85%VO2Max are still burning 75% fatty acids and 25% glucose on average, compared to people that are burning a much higher rate of glucose at the same degree of effort. This means that the cross over where the body consumption changes from one substrate to another one, has shifted in favour of fatty acids in Fat Adapted people. In a nutshell FA people are able to utilise 2-3 times more fat for energy then carbo adapted people, given that the effort isn’t maximal (highly anaerobic)9,10..
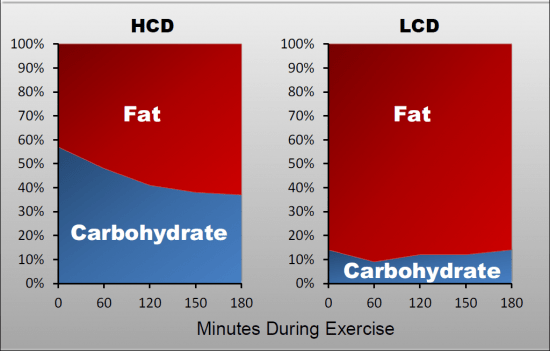
HCD = high carbohydrate diet. LCD=Low carbohydrate diet fat adapted (FA)
To my total surprise, my morning HRV baseline, given the same intensity and volume of training, improved by +12%, HF and LF also improved. Resilience to self-reported stress maintaining the same stress load improved, alongside the very predictable variables like glycaemia and ketones. This was great news especially because at least half of the group, including myself, was very prone to the dreaded OTS. Gradually, training could be performed a little more often, slightly faster and/or slightly harder/longer. Given the same effort in performance, the heart rate was around 5 to 6 bpm lower then prior to the KD, meaning that at the same working HR the energy output was slightly greater9,10. Overall we are talking of small improvements yet when combined they can produce a considerable impact.
There are various reasons why this could have happened. How KD and KAD can positively affect inflammation and to a degree sympathetic activation, is summarised below:
Reduction in inflammatory response and risk of chronic degenerative disease8
- Improved mitochondrial efficiency
- Improved Cardiovascular function
- Improved energy performance
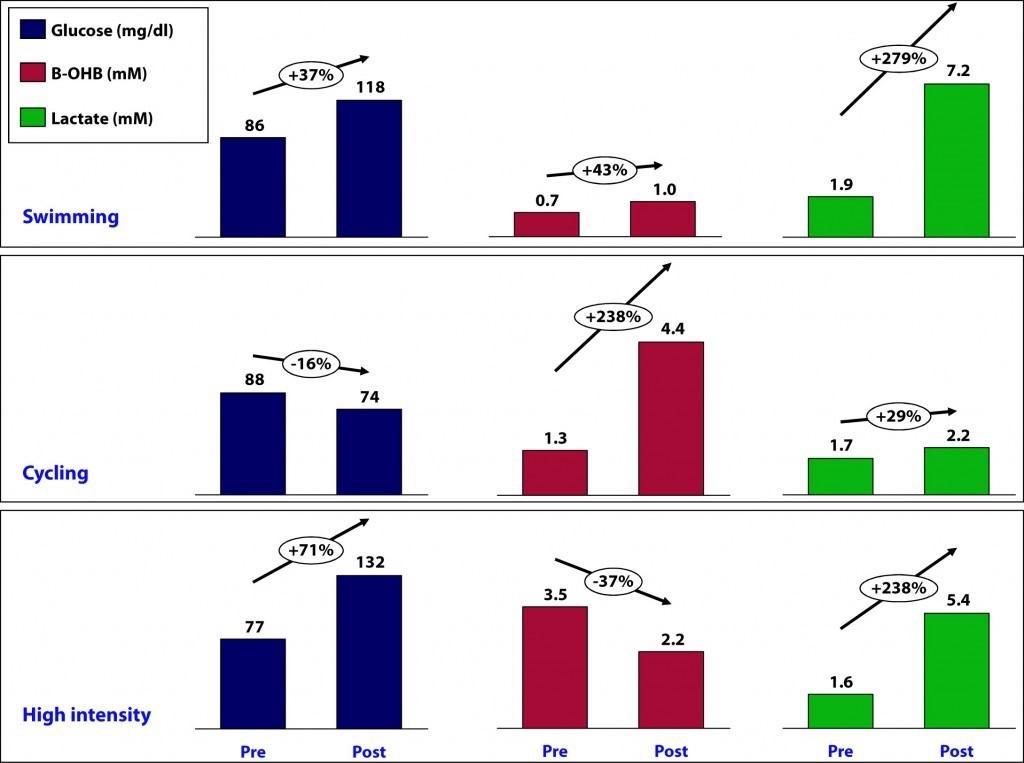
Let’s look at what happened within the anaerobic study group. When performance was close to maximum HR with high intensity performance lasted longer than 45 – 60 minutes, results were slightly disastrous! Participants complained of feeling empty, low and reaching exhaustion very quickly. The following picture represents an experiment from Dr Peter Attia and other researchers that reflect very well on my personal findings:
This was frustrating to say the least. I also fell within this subset – my sports being mostly karate and judo. After some experimentation I started to use a formula based on a proportion of Max HR during the exertion. I simply split the time spent in anaerobic and aerobic, feeding the time spent in anaerobic energy with a carbohydrate solution and using fats for the remainder of time spent in an aerobic state. It worked. In order to reproduce this strategy, you can be as empirical or as precise as you wish. You can either take in consideration heart rate training zones, estimating when aerobic effort will set in by using age and resting heart rate. Or for greater precision, you can test VO2Max/CPex with anaerobic threshold. In my experience, the difference is negligible as once the body is FA the consumption of fatty acids for energy increases, meaning that the cut-off point where the body would switch to burn just glucose changes.
As an example, in a session requiring 2 hours’ effort, a person will intermittently spend 40 minutes in an anaerobic state and the remaining time of 80 minutes in an aerobic state. I use carbohydrates for the 40 minutes with a glucose solution and fats for the rest of the time. Depending up on the sport, I worked out the energy expenditure per hour (or look at previous training data for the same type of training) for both HR bands and divided by 4 to work out the grams of carbohydrate. I then divided the energy expenditure for the aerobic time by 9 to find the grams of fats.
I split my anaerobic trial group into two – one using this method of KAD and the other one kept on a standard KD. The group on the KAD started to see real improvements similar to the aerobic group. Even when we were using carbohydrates immediately pre-workout, during the workout and as replenishment at the end of the workout alongside protein and fats, the KAD group was able to get back into ketosis is in a matter of a few hours (even for blood ketones ß-Hydroxy Butyrates (ß-HBA)). Recently I have been experimenting with super starch as this has very little impact on insulin/glucose levels and yet can provide the carbohydrate necessary for very intermittent anaerobic effort. So far the results are very promising.
Not fully satisfied with the extent of my experiments, I decided to add intermittent fasting into this conundrum. I tested out a fasting period of 16hrs+ – overnight and the duration of the morning. In discussions with Dr Justin Roberts, we have both noticed that body fat percentage dropped an average of 3% in already lean individuals, and an average of 1.5% in individuals with body fat percentage sub 10%. At the same time, we saw an increase in the ratio between lean to fat mass which I assume is a mix of increased glycogen storage and some lean mass. Pretty impressive!
At this stage I would like to clarify a couple of things with respect to substrate levels, protein carbohydrates and fats:
- Protein:
In order to maintain ketogenesis it is important to control levels of protein. General requirements range from 1.3gr/Kg mass for aerobic low impact sport to 2.0+gr/Kg mass from anaerobic high impact sports divided across meals throughout the day8. My findings revealed that we can drop 0.2gr/Kg mass and 0.5gr/Kg mass for their respective requirements. As you may know some of the amino acids contained in proteins can enter gluconeogenesis and the body seems to prefer that path when glucose is low. I had concerns that a reduction in protein could impact on recovery, immunity and tissue repair/regrowth, but in actual fact these effects were either unchanged or improved as long as individuals stayed on a KD or KAD.
- Carbohydrate:
Limited to 30-50g per day as a baseline – all from vegetables except for the extra super starch carbohydrates used in training when this was applicable (anaerobic effort).
- Fats:
Our aim was to have between 150 to 220 g of fats per day. These were mixed of healthy saturated fats, mono and poly unsaturated fats obviously also including ample essential fatty acids.
Venturing into ketosis has been a challenging experience for my group, and myself however the benefits that we have started to glean have made our efforts fully worthwhile. I hope that this article can provide you with the inspiration and information to help you to also explore KD and KAD.
By Alessandro Ferretti Dip ION mBANT NTCC CNHC. Alessandro has practiced for many years as a part of a multi disciplinary medical team at the Centre for Health and Human Performance (Harley Street, London UK) and from Tudor Medical Group (Stratford Upon Avon UK). He is a regular lecturer at UK Nutrition and Naturopathic colleges and speaks internationally on the subject of Health and Human Performance. He is currently collaborating with other International researchers on Ketogenic applications in health, Nutrigenomics, Heart Rate Variability and environmental influences on performance. Alessandro maintains a very active sport practice in Judo, Karate and Cycling.
References
- Maciej Gasior, Michael A. Rogawski, and Adam L. Hartmana Neuroprotective and disease-modifying effects of the ketogenic diet Behav Pharmacol. 2006 Sep; 17(5-6): 431–439
- Vanitallie TB, Nonas C, Di Rocco A, Boyar K, Hyams K, Heymsfield SB Treatment of Parkinson disease with diet-induced hyperketonemia: a feasibility study. 2005 Feb 22; 64(4):728-30.
- Marsh EB, Freeman JM, Kossoff EH, Vining EP, Rubenstein JE, Pyzik PL, Hemingway C The outcome of children with intractable seizures: a 3- to 6-year follow-up of 67 children who remained on the ketogenic diet less than one year. 2006 Feb; 47(2):425-30.
- Brandon KW& Hartman AL, The Ketogenic Diet: Uses in Epilepsy and Other Neurologic Illnesses Curr Treat Options Neurol. 2008 10(6):410-419
- Swain DP, Abernathy KS, Smith CS, Lee SJ, Bunn SA. Target heart rates for the development of cardiorespiratory fitness. Med Sci Sports Exerc. January 1994. 26(1): 112–116.
- Tanaka, H., Monhan, K.D., Seals, D.G., Age-predicted maximal heart rate revisited. Am Coll Cardiol 2001; 37:153-156.
- Venables MC, Achten J, Jeukendrup AE. Determinants of fat oxidation during exercise in healthy men and women: a cross-sectional study. J Appl Physiol. 2005 Jan;98(1):160-7.
- Campbell B, Kredier RB, Ziegenfuss T, La Bounty P, Roberts M, Burke D, Landis J, Lopez H, Antonio J Internatioanl society of sports nutrition position stand: Protein and exercise J Int Soc Sports Nutr. 2007 ; 4: 8. Published online 2007 Sep 26.
- Cox, P.J. & Clarke, K., 2014. Acute nutritional ketosis: implications for exercise performance and metabolism. Extreme physiology & medicine, 3(1), p.17. Available at: http://www.extremephysiolmed.com/content/3/1/17 [Accessed September 16, 2015].
- Volek, J.S. et al., 2015. Metabolic characteristics of keto-adapted ultra-endurance runners. Metabolism. Available at: http://www.metabolismjournal.com/article/S0026049515003340/fulltext [Accessed November 8, 2015].
Further References
- Gillies at al (2008) Journal of nuclear medicine: Society of Nuclear Medicine vol. 49 Suppl 2 p. 24S-42S
- Quillin, 2005; Calvo et al, 2010; Klement & Kammerer, 2011.
- Shimazu et al.(2013) Science (New York, N.Y.) vol. 339 (6116) p.
- Masino, Susan A.; Rho, Jong M. Mechanisms of Ketogenic Diet Action (2012) National Center for Biotechnology Information (US)
- Haces ML,et al Exp Neurol. 2008;211(1):85-96. doi:10.1016/j.expneurol.2007.12.029.
- Julio-Amilpas A,et al J Cereb Blood Flow Metab. 2015;35(5):851-860. doi:10.1038/jcbfm.2015.1.
- Finn PF, Dice JF. Ketone bodies stimulate chaperone-mediated autophagy. J Biol Chem. 2005 Jul 8;280(27):25864-70.
- Douglas C. Wallace, Weiwei Fan, and Vincent Procaccio. Mitochondrial Energetics and Therapeutics Annu Rev Pathol. 2010; 5: 297–348.
- Oliver E. Owen “Ketone Bodies as a Fuel for the Brain during Starvation” Biochemistry And Molecular Biology Education.Vol. 33, No. 4, pp. 246–251, 2005.
- Santos et al.(2012) International Association for the Study of Obesity vol. 13 (11) p. 1048-66.
- Dashti et al. Beneficial effects of ketogenic diet in obese diabetic subjects. (2007) Molecular and cellular biochemistry vol. 302 (1-2) p. 249-56
- Kashiwaya Y et al Substrate signaling by insulin: a ketone bodies ratio mimics insulin action in heart. Am J Cardiol. 1997;80(3A):50A – 64A.
- Pr Jeff Volek IHMC
- Jones RG, Thompson CB.Genes Dev. 2009;23(5):537-548. doi:10.1101/gad.1756509.
Great stuff Alessandro!
thank you Marco, much appreciated from a scientist like you.
Interesting stuff. I coach a sprint swimmer (short sprint 50m). What is the view on LCHF diets for sprinters? Intuitively I would expect it not to be ideal for sprinting but there seems to be an argument for other health benefits. Do you know of any research on anaerobic performance with this diet?
Hi Martin,
Great that you found the article interesting. I practice 2 sports where mainly Type 2b muscle fibre are activated (Judo and Karate). Similarly for your swimmer and correctly as you say is that it can be tricky/at times not suitable in using ketogenic diet or keto adapted diet (with carbs back loading).
From what I gather in my experience and the clinical data that is out at present you have a few options:
1) keep as you are and obviously you won’t get the benefit
2)enter full ketosis and go through the adaptation period (with full benefits mitogenesis, recovery etc…)
3) use a modified version (adapted) where you carb back load in the evening to ensure replenishment of carbs for the following day.
this all depends by the HR sustained during the sprint and how long for. I understand that is in the mid 20’s so normally the body will store plenty of resources to keep up with that demand. Also KD helps in up regulating Cori cycle for the regeneration of substrate (lactic acid back into energy) when the O2 is low and this can be very useful during training session where multiple efforts are performed. After I have been fully adapted (with interesting failures in my experiments at the start….) I now only have the carbs that I find in low carb veggies, and I have a lot of these. Yet my total NET carb (meaning total carb – fibre = net carbs) intake for the day won’t exceed normally 50gr. In this way I get the whole benefit of the KD but I also have the ability to perform better including anaerobic. Interestingly seems that my lactic acid threshold has moved up considerably and also my recovery between spikes (in your case sprints and in my case sparring sessions) in the same training session is grammatically reduced/improved. The body seems to be able to adapt very well.
One thing I should say, it’s not an easy diet to get the head around so initially things can be difficult. Normally in physically very active people (and healthy people) the adaptations is much shorter. During the transition training quality can go inconsistent but persevering will normally resolve the issue in few weeks. I would suggest try this approach away from important competitions and event, just to make sure. In sport I normally suggest to make sure that monitoring of ketones and glucose is consistent and also using aids like MCT oils exogenous ketones.
Hope this helps
Great article! Have you performed any shorter higher intensity runs (5k, 10k) since fully adapting? If so, how did you those feel? Thanks!
JT,
LOL, yes I did short term (very) high intensity exercise (like multiple sprints and consecutive sparring sessions) and short high intensity bike rides and when I got my carbs/MCT refuelling wrong… we’ll, went very wrong. I tend to allow the patient to be guided by how they feel once fully fat adapted ideally measuring glucose (blood) and ketones (breath and blood). There is a big difference between people on a high(er) fat diet and people that are fully fat adapted – meaning that the latter person uses preferentially fats as the primary source of fuel with all the advantages of the case. Once people are fully fat adapted they might need carbs in much smaller quantities and only at med-high and maximal intensity to fulfil the glycogen stores once these are depleted -refuelling need to start before the glycogen stores are depleted). I have found for example that if I have such a session I only need no more then 20-30grams of a mix 2:1 maltodextrin to fructose (and either ketones/MCT pwd) to maintain prolonged effort. If the session is less then 1-1 1/2hrs or low intensity then I just have water/electrolytes. An important point is to start with your glycogen stores up, meaning refuelling well the night before and have maybe small amount of super starch 1h before the session. So, in these cases the performance was great and person was able to carry out very efficiently (if not better) the session. When people were not fat adapted and any of the other variables were out, then they didn’t feel great. I would suggest that if you have an important session, stand down from trying anything new, whereas if you have some time like 2-3 months to experiment, then go for it.
Hi Alessandro,
Sorry to comment on an old post. This is a fascinating article and I would like to know what you think.
I’ve been on the KD for over three months now and am pretty confident that I am fat adapted (I test breath ketones regularly). I have been tracking my HRV scores pretty regularly for a few years now and track my HR during workouts. I box recreationally and do some other stuff.
I have noticed an increase in my overall HR during workouts—spending a lot more time in the anaerobic range and often exceeding that range than before I started the KD. So, for instance, my workout yesterday was about an hour with my HR falling 58% in the anaerobic range, and 20% in V02 Max range, with only 22% falling in the aerobic range and below. Incidentally, my HRV score has been consistently and sometimes significantly lower in the last three months compared to pre-KD. My typical boxing workouts are about an hour in length, sometimes longer, with additional morning workouts that last about 30 minutes (these are usually HIIT stuff or lifting).
I should also add that my fatigue during workouts has dramatically decreased in more recent weeks compared to the first six weeks or so of being on the KD. But still not where I was before doing the KD.
I’m wondering, after reading your article, whether I should not be supplementing with superstarch. I already supplement with electrolytes. Any suggestions or advice?
Hi Josh,
No problem re reply to an old post. What you are experiencing is totally in line with some individuals. I obviously do not have any specific data re diet (quality, macros and nutrition density), lifestyle etc so I will have to make few assumption and I’ll mention a few things that you could look into.
The first is def associated to the type of effort and KD applications. Many people doing high volume low intensity effort or lifting tend to do pretty well in the right context. The problem comes more with the type of activity you do (same for me doing karate and judo) when especially in sparing session we need to access glycolysis. At that degree of intensity and O2 availability (heavily reduced) fats and ketones might just not be enough to support the demand from the body. I suggest that you do training session fasted to train your body in using more substrate from fats yet at the same time when you push, have a context or hard training you might wish to use some carbs to support energy production system relative to the effort. Generally 30-50gr a day on that day should be enough but you need to experiment.
The other aspect is that carbs are potentially needed for recovery, well, indirectly at least. IN the recovery phase of the resolution of the inflammatory response IGF-1 and insulin are needed to ‘resolve’ inflammation. I have found that many athletes that do not have adequate (good luck to anyone defining that….) intake of carbs might not induce the same degree o inflammation but at the same time they might not recover as fast.
I suggest you play around with these and if you struggle get back to me.
Hi Alessandro,
Awesome article, Im applying this and feel great!
Im a martial artis actor and I been doing KD for 3 years. I measure my blood ketones and acetone and have lots of info.
This last year Im been mainly on a Plant based KD and will like to see if there is a way to talk to you about this and see what you think.
As an martial artist /actor my goal is performance but at the same time need to have some muscle and look rip.
I have lots of info from these 3 years that will like to discuss with you.
Fat ratios and cholesterol results on traditional KD vs Plant base KD.
Hope we can coordinate a skype talk!
Im a big fan!
here is a demo of what I do,
https://www.youtube.com/watch?v=3e2xs4dvp9I
Hi Marko,
Thanks for the comment, and glad you are enjoying Alessandro’s analyses!
He is currently recovering from recent knee surgery so you might not get a reply quickly, but hopefully he can get back to you when he’s back to full strength.
best,
Simon.